|
|
|
|
|
|
Hello ,
As we are now entering the sixth month of the Covid-19 health crisis, I can sense the tide shifting, the pendulum swinging back.
How about at your organization? Are people thinking more strategic, more proactive about the new situation?
Maybe it’s that we’ve been with this “new normal” for "so long" and as impatient and creative people, we just have to move on and move forward.
We don’t do “stagnant”, especially not in the US.
Whatever it is — the interest in using outside expertise in getting telehealth right (which is what we at Ingenium specialize in), is increasing and we are ready!
Over the course of many conversations and webinars I also picked up that organizations are looking beyond video visits or telephonic “care” — to remote patient monitoring, or RPM.
In this week’s article I cover the basics of using RPM for readmission prevention, which, when done right, is saving health systems hundreds of thousands of dollars per year, along with some other considerations for “post-acute care”.
In future articles, I’ll also cover the use of RPM for chronic disease management but also stay focused on the home as we explore “the hospital at home”.
What are your organizations’ plans for RPM?
With kind regards,
|
|
|
|
|
P.S.: Don’t miss this week’s webinar on “Measuring Telehealth Success” - to the point of the first mindset in today’s article.
|
|
|
P.S.: Do you know a colleague who might enjoy reading this newsletter? Please send them this link to see an archive of past newsletters and an opportunity to subscribe:
|
|
|
|
|
|
|
Telehealth for Post-Acute Care
|
|
|
Telehealth is often thought of as a tool to conduct video visits
for “regular”, non-acute care. A few weeks ago I covered a number of use cases for telehealth within the hospital and in this article we’ll be looking at the various scenarios where telehealth can be of use for post-acute care.
Telehealth, Telemedicine and Remote Patient Monitoring
Before we dive into the application of telehealth for post-acute care, let me share with you my now 10-year old definitions for telehealth and telemedicine.
Telehealth is “Delivering Care at a Distance”, i.e., any interactions modern healthcare consumers (a.k.a. patients) have as part of their care. This includes features mostly provided through the meaningful-use mandated “patient portals”, such as scheduling appointments, reviewing physician notes, immunization records or lab results. Telehealth at this level also includes any education patients
receive as part of their pre-surgical or post-surgical preparation or related to their diagnosis.
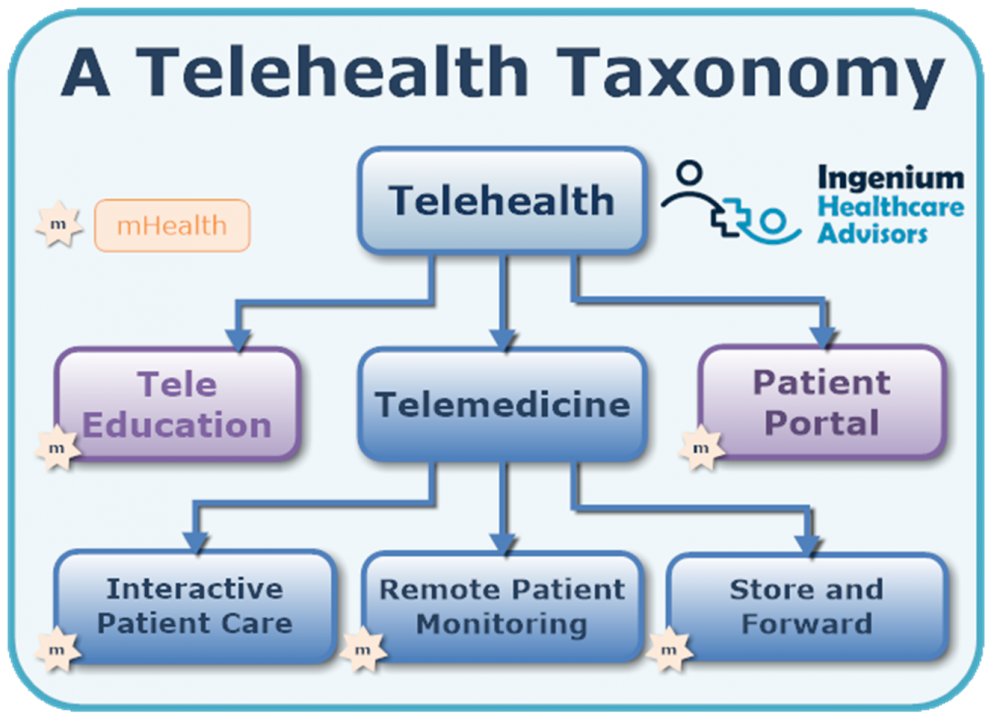
Telemedicine is “Practicing Medicine at a Distance”, i.e., the interactions of clinicians with patients such as live, interactive patient care (a.k.a. video visits or telephonic telemedicine), the review and monitoring of vital signs (a.k.a., remote patient monitoring) and the review of asynchronously received information (a.k.a., store & forward) such as a picture of a skin lesion or a faxed EKG.
When we put this all together as a taxonomy, a picture like this emerges:
|
|
|
|
|
|
|
Thus telemedicine comprises video visits, text-based care, telephonic visits, remote patient monitoring and store and forward as the various modalities to enable clinicians to “practice medicine at a distance”.
The High Cost of Readmissions
The first, most-commonly used scenario in post-acute care is the use of remote patient
monitoring for readmission prevention. Within the Medicare population, about 1 in 6 patients gets readmitted within 30 days.
With many payors not reimbursing for readmissions occurring within 30 days of discharge and with Medicare imposing a penalty (which in 2019 affected 83% of hospitals), the financial incentives for preventing readmissions are high. The readmission improvement initiative focuses mostly on patients with a diagnosis of heart failure (CHF), COPD, acute myocardial infarction (AMI or heart attack), and a few other diagnoses.
While the penalties only apply for Medicare (though it affects ALL of the hospitals’ Medicare payments), the higher return on investment into readmission prevention actually comes from the savings of the variable cost associated with a readmission, oftentimes in the range of $6,000 to $9,000 dollars for most of my clients.
Just saving 1 readmission a week can yield savings of over $250,000 in a year,
easily justifying the investment in establishing and the operational cost of running the program. Some initiatives programs show returns of over 13:1, i.e., that for each $75,000 invested, $1M were returned in overall savings.
And this is only the financial side. From a clinical perspective, a readmission interrupts the healing process of patients - including the impact of a repeat admission on family members. Obviously readmissions also lead to longer recovery and rehabilitation times.
The first set of tools of reducing readmissions focuses on the standard improvement interventions, such as optimizing the discharge process, a focus on medication reconciliation, proper care transitions into home care, etc.
Another set of interventions looks at the 30-90 day period after discharge by monitoring the patients’ key vital signs: remote patient monitoring.
Remote Patient Monitoring for Readmission Prevention
Remote Patient Monitoring, or RPM, provides patients with a kit of monitoring tools that allow the collection of key vital signs on a daily basis. The most common tools these days include a blood pressure cuff, a scale, a pulse oximeter, and, for diabetic patients, a glucometer. Many RPM kits also include a tablet for daily prompts,, daily questionnaires (such as a PHQ 9 for assessment of depression) and video visits.
Most vital sign tools are connected wirelessly using Bluetooth or other wireless connectivity technology. All the patient data is periodically and securely sent to a central database “in the cloud” and presented to the monitoring nurse in an RPM-optimized dashboard.
|
|
|
On a daily basis a monitoring nurse, who can track about 120-150 patients simultaneously, reviews any missed vital sign connections or deviations from the normal parameters and reaches out to the patient. If warranted, the monitoring nurse escalates the patient to their primary care provider for further evaluation, such as the adjustment of medications.
The best performing remote patient monitoring programs, however, make systematic use of the video chat capability to reach out to patients directly. One of my clients for example puts the patient in touch with the pharmacist for post-discharge medication reconciliation. Connecting social workers, mental health professionals or
hospice specialists with the patient is also a very valuable use of the infrastructure now available in the patients home.
Some solutions also offer pre-designed questionnaires, asking about activities of daily living (ADLs) or other questions related to the discharge diagnosis.
Post-Acute Care in Nursing Homes
Another set of common use cases and valuable services arise from establishing a tele-connection with nursing homes. Once the technology to do a video visit with nursing home residents is available, numerous post-acute care scenarios arise, including:
post-discharge transition (e.g., nurse to nurse or physician to medical director)
medication reconciliation with pharmacists
pre-admission evaluation and triage
Remote Patient Monitoring oftentimes does not play as big a role as in a discharge to a patient’s home, since the nursing home’s staff typically monitors and manages the key vital signs. However in understaffed nursing homes or in nursing homes affected by Covid-19, RPM as described above can still present a useful solution under the right circumstances.
Telehealth and Post-Acute Care
While Telehealth was initially conceived for giving patients better access to care, especially in rural areas, the dramatic advancements in technology make it absolutely feasible to collect data of high clinical quality in a reliable manner.
While the first article in this series focused on the acute care scenarios in the hospital, in future series of articles we’ll also be looking at the “hospital at home”, how not only readmissions but also admissions can be prevented using today’s solutions in the proper way.
RPM is frequently mentioned these weeks as a technology of high interest, especially when it comes to its use for effective chronic disease management. But that is a topic for yet another
article.
|
|
|
To receive articles like these in your Inbox every week, you can subscribe to Christian’s Telehealth Tuesday Newsletter.
Christian Milaster optimizes Telehealth Services for health systems and physician practices as Interim Telehealth Program Director. Christian is the Founder and President of Ingenium
Digital Health Advisors where he and his expert consortium partner with healthcare leaders to enable the delivery of extraordinary care. Contact Christian by phone or text at 657-464-3648, via email, or video chat.
|
|
|
|
|
This edition of Telehealth Tuesday was sent to _t.e.s.t_@example.com.
Ingenium Consulting Group, Inc., 1173 Bayview Vis, Annapolis, MD 21409, United States
If you no longer wish to receive weekly updates, I'm sorry to see you go. Unsubscribe
|
|
|
|
|